Explainers
21 MIN READ

We have not dealt with a disease like COVID-19 in over 100 years.

Click image for enlargement. Source: Government of Nepal, Situation Report 40, Situation Report 39
We have not dealt with a disease like COVID-19 in over 100 years.[1] Given the global scenario, it is only a matter of time before a case is detected in Nepal again. We neither have the diagnostic capacity, nor the intensive care infrastructure to handle a potential outbreak. These capacities are not built overnight, and we should expect the worst and act accordingly.
However, there are still things we can do as individuals to minimize harm. There are also things we should demand from our government. In light of the risk looming over Nepal, it is imperative that each individual needs to take care of themselves, their families, and their communities. We need to start social isolation immediately, stop going outside if we experience any symptoms, and support each other throughout this ordeal. We also need to be aware of what services are available to us, how to make use of them, and how to make them better.
Explore references if you have time, if not please go through the highlighted section.
At this stage, according to Singapore’s Minister of Foreign Affairs,Vivian Balakrishnan, “Maps which do not reveal any cases, probably are indications of lack of testing.” To put it in context, Nepal is the only country on earth to have diagnosed a patient in January and then have no following cases.[2] Most countries that have single digit cases only started reporting in March. All our neighbours have increasing caseloads—we are an anomaly both regionally and internationally. Thus it is highly likely that the reason why we are not seeing cases is because we are not diagnosing enough. This is aggravated by reports of improper management for those seeking diagnosis [3] and widespread doubt on diagnostic facilities [4].
Furthermore, there are certain cases of COVID-19 linked to Nepal that have not been followed through properly, or information regarding contact tracing investigations have not been made transparent enough. The first patient reported on January 13 was a student returnee from Wuhan. Even though he recovered, neither the government nor a recent correspondence regarding his case in the Lancet detailed whether or not contact tracing was done.[5] This means that we are not sure if the family and friends of the person who contracted COVID-19 were tested for the disease.
Similarly, no information is available with regards to contact tracing for two other COVID-19 cases. Through autopsy it was identified that a 69-year-old man with prior travel history to Nepal died in Spain on February 13,[6] there is no report consequently in Nepal regarding whether or not follow-up investigations were done in the hotels or places he visited. Furthermore, a man in Tasmania, Australia who arrived in Hobart on February 26 was diagnosed with COVID-19 after a trip to Nepal.[7] Even though he transited through Singapore and Sydney after leaving Kathmandu, it cannot be ruled out that the virus could have been contracted in Nepal. There are no reports regarding whether or not contact tracing was done in this instance as well. These are grave discrepancies on part of the Government of Nepal.[8]
According to the current algorithm for diagnosis, the priority is still symptomatic people with travel history to affected regions or those in contact with such individuals.[9] Given that affected areas now include over 100 countries and with the added information that the disease could be spreading during pre-symptomatic conditions [10] there is an urgent need to broaden who is getting tested.
The other thing to keep in mind is the exponential growth trajectory of COVID-19. We know from estimates that in China an infected individual could have transmitted the disease to around 2 other individuals [11], and that the disease initially doubled every 7 days [12]. Things can get out of hand very fast.
More importantly, in Nepal, even when a second case gets detected the situation can be far worse than it seems. This is because the initial number of diagnosed cases does not reflect the actual number of active cases in any country.[13] For example, in a study conducted by the Chinese Center for Disease Control and Prevention it is estimated that when Wuhan was put under lockdown on January 23 there were only 444 detected cases from the day before; however, upon surveying patients on when their symptoms actually started, there were around 12,000 actual cases on that very day.[14] So just because one more person is diagnosed, it does not mean that only one more person has COVID-19; there can be many more actual cases that have not been detected.
This brings us to Nepal’s diagnostic capacity. Currently we only have the National Public Health Laboratory in Teku testing for the coronavirus using real-time polymerase chain reaction (RT-PCR). At a time when providing tests to more people is the number one priority, there should be minimal logistic and bureaucratic hassle to do so. Expanding diagnostic services to multiple laboratories, both public and private, is imperative. We cannot just be running 17 tests a day anymore.[15]
This is particularly important because it is not possible to decentralize diagnostic services, as not all provinces in Nepal have facilities required to conduct a RT-PCR. Kathmandu is still the only place in the country that can run these tests. And according to a statement made by Dr. Runa Jha of the National Public Health Laboratory, it will take over a year to develop such facilities outside the capital.[16]
There is another complication, samples for the test such as throat swabs require a viral transport medium (VTM), which needs to be maintained at a cold chain of temperatures between 2 and 8 degree Celsius.[17] Not all clinics and hospitals have VTMs. The government needs to make public a list of all hospitals capable and authorized to collect and send samples to Teku using VTMs, especially because it is recommended that those seeking diagnosis should not directly go to a hospital but call in advance.
It has been reported that as of March 19, 2020 there were only 1,500 COVID-19 test kits remaining in the country.[18] In the event that there is another case, we need to be prepared to diagnose as many people as possible, while prioritizing contact tracing. 1500 kits is not sufficient to do this. While plans exist to get more kits and manpower for testing,[19] this is not specific enough. We need to know the exact date of arrival, the number of kits ordered, and when tests will be available to more people. There should no longer be any confusion with how diagnosis is being done. The Government of Nepal could hold its ground, if it did everything possible to conduct enough diagnoses using scientific sampling techniques, in order to say that we do not have any more cases of COVID-19. However, given the current context, it is not possible to say so.
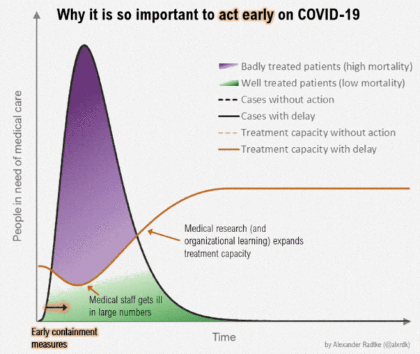
There are two important things to keep in mind during the COVID-19 pandemic. Firstly, how fast the disease can spread. Secondly, how many cases a health system can handle. To “flatten the curve” means to spread the infection of the disease over a longer duration of time so that the health system is not over burdened. This can potentially save more lives, even though a similar number of people get infected.
We know that COVID-19 can spread really fast, so what about the capacity of the Nepali health system? We must realize that Nepal is very different compared to those countries that are currently facing the crisis. Italy for example has 3.2 hospital beds per 1000 people and the United States has 2.8.[20] In comparison, Nepal only has around 0.9 hospital beds per 1000 people.[21] If the health system of high income countries were not prepared for COVID-19, we are not prepared at all.
This data is also inclusive of all hospital beds. In terms of intensive care units (ICUs) the Government of Nepal is only planning on adding around 200 beds.[22] Which means that, even with existing ICU capacity, Nepal is only able of managing a few hundred severe patients of COVID-19 at best.[23] Keep in mind that Italy has around 5,200 intensive care beds and is still struggling.[24] Indeed, there are plans to increase bed capacity, but in the event of an outbreak of the scale we are witnessing in Europe or East Asia, we will not be able scale fast enough. This is not something you can do in a few days or weeks, it requires years of investments in the health system to develop advanced intensive care facilities.
This is where social distancing comes into play and why it is extremely important. The Government of Nepal is taking the appropriate steps at the moment in this regard.[25] We as individuals living in Nepal need to do everything possible in our own capacities to ensure that this disease does not spread. Social distancing is fundamentally important so that the possibility of COVID-19 spreading is reduced, and in effect less people die. Current mortality estimates vary. Areas that diagnose faster and have enough hospital beds for patients fare better: for example, South Korea has an estimated case fatality rate of only 0.9%; whereas in China the mortality rate was estimated to be 4%; and in Italy it is nearing 8%.[26] We honestly do not have the data to say what the mortality scenario will be in poorer countries such as Nepal.
In light of this, public activities need to stop now; schools and offices need to close; and we all need to cooperate. This is necessary in Nepal, even though active cases have not been detected; our health system is inherently weak and cannot handle any outbreak of this scale. Taking extra precaution is not only advised but necessary. It is not an exaggeration to say that in Nepal we cannot even afford to have a curve, let alone flatten it.
There is one more thing that we all need to demand for—information. The current communication strategy for COVID-19 in Nepal is not streamlined. While the Health Emergency Operation Center portal is a good start, it is not good enough. The Government needs to streamline all communications, reports, and data, including those of the high-level committee on COVID-19 headed by Deputy Prime Minister Ishwar Pokharel. Information regarding when, where, and how to get a diagnosis needs to be spelt out for everyone to understand. A proper list of all hospitals authorized to take care of COVID-19 patients, and the protection offered to medical care providers, also needs to be public. Transparency of data regarding the number of tests done and the number of positive cases is of utmost importance. In order for the public to not panic, we need to know that we can trust the information we are receiving at all times. This is not a lot to ask for, and it is after all our constitutional right.[27]
To conclude, here is a pertinent quote from Dr. Tedros Adhanom, the Director-General of the World Health Organization:
In the past week, we have seen a rapid escalation of cases of COVID-19. More cases and deaths have now been reported in the rest of the world than in China. We have also seen a rapid escalation in social distancing measures, like closing schools and cancelling sporting events and other gatherings. But we have not seen an urgent enough escalation in testing, isolation and contact tracing – which is the backbone of the response. Social distancing measures can help to reduce transmission and enable health systems to cope. Handwashing and coughing into your elbow can reduce the risk for yourself and others. But on their own, they are not enough to extinguish this pandemic. It’s the combination that makes the difference.[28]
आपतकालीन नम्बरहरु । Emergency Numbers:
COVID-19 Toll Free Hotline (6am–10pm): 1115
For questions on diagnosis (8am–8pm): 9851255834, 9851255837, 9851255839
Nepal Ambulance Service: 102
उपयोगी नेपाली स्रोतहरू | Useful Nepali Resources:
अन्तर्राष्ट्रिय स्रोतहरू | Global resources:
मेडिकल जर्नलहरु । Medical Journals
Most medical journals are providing COVID-19 related research articles for free:
::::::
Author's note: I want to clarify that I am not a doctor and am not authorized to give medical advice. I work in the field of public health policy and research. For medical advice please call the numbers provided above or contact your nearest hospital/clinic. And because I also practice social media distancing, I want to request you to email me in case you have further questions: priyankarbchand@gmail.com
I will try to update this document as more resources become available, and as the situation changes in Nepal.

Priyankar Bahadur Chand Priyankar Bahadur Chand is a researcher, public health activist, and archivist based in Kathmandu and Dhangadhi. He is the co-founder of Sickle Cell Nepal, a non-profit organization which works to improve the access to health services for patients of hemoglobinopathies in Nepal.

COVID19
Features
3 min read
To lessen the load on the country’s hospitals, the government has asked that people go to the hospital only for medical emergencies
COVID19
News
3 min read
The government will need more vaccines and the funds to buy them to meet its immunisation goals
COVID19
News
4 min read
A daily summary of Covid19 related developments that matter
Features
COVID19
6 min read
The popular tourist destination of Ghandruk was hit hard by the pandemic but locals first turned to farming and then to domestic travelers to survive.
COVID19
Features
3 min read
The infection count could double in 20 days--such numbers could break the country’s health system
Features
14 min read
Menstrual education in Nepal is woefully inadequate and, at times, actively harmful, posing risks to health while reinforcing existing stereotypes and stigmas.
Perspectives
8 min read
There are strong links between economic stressors caused by climate change and child marriage around the world. A spattering of evidence suggests this is a serious problem in parts of Nepal as well.
The Wire
19 min read
Food poverty is on the rise in rich countries. And evidence suggests the impact can last for years afterwards.
